
“Words are important. If you want to care for something, you call it a “flower”; if you want to kill something, you call it a “weed”.
(Don Coyhis)
At Provide, our central driving value is the belief in the fundamental and inherent worth of all people—including those who cause us discomfort. Often, this discomfort is a product of stigma: the negative view we hold of people because of a certain quality or circumstance. As providers of abortion referrals trainings, working with partners in fields that include domestic violence, sexual assault, HIV, and substance use disorder, stigma sits at the forefront of our work as well as that of many of our partner sites. Only by recognizing and working against stigma can we create systems that can truly provide patient-centered care for our clients. Our blog series on stigma discusses how it shows up in health care and social service delivery; how to identify signs and symptoms of stigma at the individual, environmental, and structural levels; and how to contribute to a stigma-free workplace.
How to Identify Signs and Symptoms of Individual Stigma
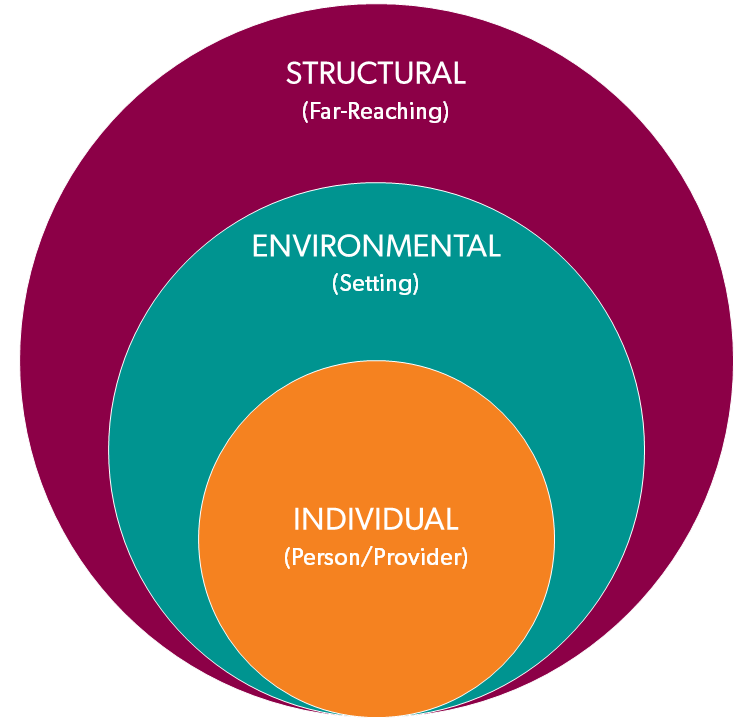
In seeking to identify where stigma might be present in your professional setting, it can be helpful to think about stigma as occurring at three levels:
Individual: from the individual provider who is interacting with the patient/client
Environmental: from the immediate environment where health care and social services are delivered (the community or clinic in which you practice is also part of the environment)
Structural: from the immediate policies and procedures that guide how health care and social services are delivered (this can include individual organizations, as well as local, state, and federal laws and policies)
These levels are interconnected. An individual’s stigmatizing thoughts and behaviors can influence the environmental and structural levels. As individuals, it is at this level that providers have the greatest ability to identify stigma and implement change.
Stigma is complicated, and there are numerous components at play that allow stigma to affect health care and social services. One of these components is power. It’s important to realize that, where power imbalances occur, stigma has serious consequences for the lives of the less powerful. Providers and the structure of the systems where they work are the gatekeepers for services and information that impact the quality of clients’ lives. Power imbalances in the provider-client relationship can occur when the provider has more information and is in a position to share (or not share) that information with a client or another provider. Power imbalances among people, in environments, and in the structure of our system create an atmosphere where stigmatizing behaviors thrive, putting clients at greater risk for negative outcomes in a number of ways.
To reduce negative outcomes for patients and clients, providers should continuously recognize, address, and work to change inequity and reduce stigma. One way they can do so is by assessing their own power dynamics and interactions with patients/clients and colleagues. Although it may be unintentional, providers may contribute to stigma through their communication, behaviors, or actions (or lack thereof).
Communication
Language contributes significantly to stigma. Warning flags for stigmatizing language include:
- Use of slang and idioms
Avoid using slang and idioms when talking about health care conditions (see table below). These terms not only stigmatize, but also are subjective and may be misinterpreted by the patient, the next provider who reviews these documents, or by other people in different disciplines such as child protective services, the criminal justice system and courtrooms, or insurance companies. - Labeling
Examples include saying a person in crisis is “having a breakdown,” assuming a person is “scamming the system,” presuming that an overweight patient is lazy or unhealthy when they actually have a health condition, and referring to a person who uses a service regularly as a “frequent flyer.” - Negative body language
It’s not just what we say; how we say it matters too. Examples of negative body language include avoiding eye contact, staring at your chart/tablet/intake form instead of looking at the patient/client, forced smiling, standoffishness, crossed arms or legs, eye rolling, fidgeting, slouching, and frowning. - Unclear, incomplete, and vague documentation
Unclear, incomplete, or vague documentation is left up to the next person’s interpretation. For example, if a provider documents, “Jane is sexually promiscuous,” the provider is stigmatizing Jane because however many partners Jane said she had is clearly not an acceptable number to the provider. Now the next provider who reads this will make their own assumption about what this documentation means. - Inaccurate information
Providers may share inaccurate information due to lack of knowledge or stigmas they hold. Inaccurate information may be shared to discourage a person from seeking particular treatments or persuade the person to take particular actions.
Language is a tool that can be used to affirm or disparage. Use person-centered language to convey respect and honor the value of every person, instead of defining them by their characteristics, behaviors, or health condition. Below are just a few examples of person-centered language.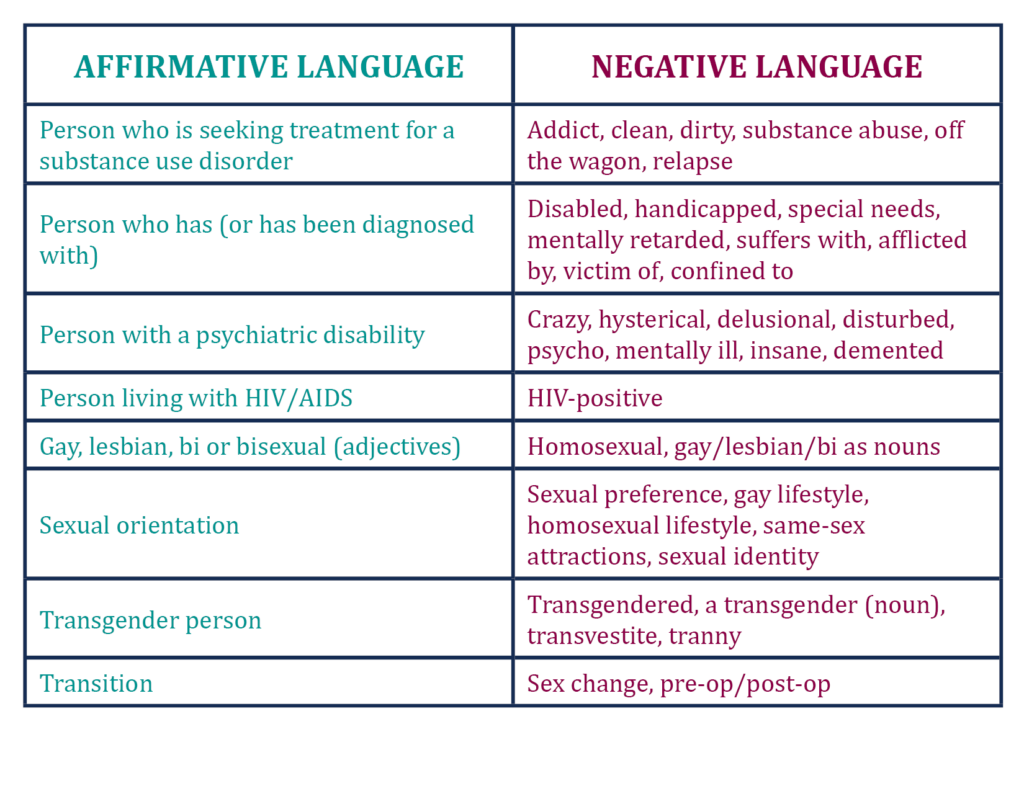 When in doubt, put the word “person” first. If you aren’t sure what language to use, ask your patients/clients what language they use to describe themselves, and then confirm that it’s okay for you to use that language too. For more resources on using non-stigmatizing language, refer to the links below.
When in doubt, put the word “person” first. If you aren’t sure what language to use, ask your patients/clients what language they use to describe themselves, and then confirm that it’s okay for you to use that language too. For more resources on using non-stigmatizing language, refer to the links below.
- Language Matters: Learn What to Say and Why | National Perinatal Association
- Resources on Perinatal Substance Use | National Perinatal Association
- Words Matter: How Language Choice Can Reduce Stigma | Substance Abuse and Mental Health Services Administration (SAMHSA)
- Language of Recovery: Guiding Principles | Julie Cole
- Language of Recovery: Terminology Guidance | The Courage Center
- Why Language Matters: Facing HIV Stigma in Our Own Words
- An Ally’s Guide to Terminology | Gay & Lesbian Alliance Against Defamation (GLAAD)
- Stigma from Professional Helpers Toward Survivors of Intimate Partner Violence | Allison Crowe and Christine E. Murray
Behaviors and Actions
Behaviors and actions that are dismissive of a person’s full spectrum of needs may also contribute to stigma. Stigmatizing behaviors and actions include:
- Inadequate or delayed treatment due to misattribution of symptoms
- Refusing to provide care, information, or treatment based on belief of the patient’s/client’s beliefs
- Having lower expectations for health outcomes for patients with substance use disorders (SUDs)
- Believing that a patient who returns to use while participating in an SUD treatment program is undeserving of treatment
- Believing that a victim who returns seeking services is undeserving of shelter
- Excluding patients with mental health diagnoses from treatment decisions or providing less treatment information
- Refusing to provide an abortion referral for a patient who doesn’t want to be pregnant
Provider communication, behaviors, and actions that contribute to stigma ultimately influence clinical interaction and treatment-seeking behaviors. When people perceive stigma from a provider, they trust providers less, experience more self-stigma and lower satisfaction, and are more likely to drop out of care earlier. These factors compound and lead to worse outcomes overall. When thinking about stigma, it’s important to take our values and personal opinions into account. Staying grounded in ethical and professional care can help us navigate uncomfortable scenarios. As individual providers, it’s up to us to do what we can to honor the worth of every person, reduce the burden of stigma, and improve access to health care.
How can you address individual level stigma in your workplace?
- Train staff on how to use a comprehensive and up-to-date list of referral resources that value patient autonomy, dignity, and worth.
- Train staff on how to recognize their biases and provide support on managing the tension that can arise when personal values conflict with professional roles.
- Provide staff with examples for how to document patient interactions without using stigmatizing language.
Previous: How does stigma show up in health care and social service delivery?
Next: How to Identify Signs and Symptoms of Environmental Stigma
